On and off again upper back pain
 Written by Judy Haluka
Written by Judy Haluka
Changes: Fix formatting of the rhythm strip
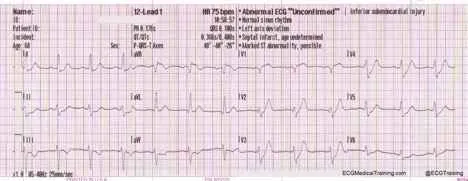
A 43-year-old female comes to her physician’s office complaining of “fatigue and some on and off again upper back pain.” Today that back pain started about an hour ago and just kept getting worse so she called for an appointment. She is sitting in the waiting room and you call her in ahead of her appointment because she looks very anxious and uncomfortable. On examination, she is pale and slightly diaphoretic. Her radial pulse is very weak. You estimate her pulse to be 90. Her blood pressure is 94/70 with a pulse oximetry reading of 92% on room air. She has rales in the bases of her lungs bilaterally. She admits to being “a little short of breath.” You ask the tech to complete a 12-lead ECG. It shows the following.
What are your actions? Do you have any concerns?
Even without the ECG, you have reason to be concerned. Women having myocardial infarction tend to present with vague symptoms like fatigue and their ischemic pain presents as back rather than chest pain. In addition, she is beginning to show signs of congestive heart failure and even cardiogenic shock. (SBP 90s and rales present in her lungs)
Her ECG seals the deal. This is a classic example of DeWinter S/T waves indicative of proximal LAD (left anterior descending) occlusion. Note the 2+mm of ST depression in the anterior leads (v1, v2, and v3) with upright symmetrical T waves. In addition, there is an ST elevation in aVR. This is only present for proximal LAD or left main trunk lesions.
Appropriate actions: You call an ambulance (if your office is not located in the hospital) and notify the receiving emergency department that you are sending an acute anterior wall infarction to them. You direct EMS to the nearest hospital with interventional cath lab capabilities because this patient will do best with immediate intervention. Because she is short of breath and her oxygen saturation is less than 94%, you place oxygen 4 liters via nasal cannula, resulting in an increase in her saturation to 97%.
You give her 4 baby aspirin (324mg PO). If there is time while waiting for the ambulance, you can start an IV. Hold nitroglycerin at this time due to her low blood pressure. She can be given Morphine 2–5mg IV repeated frequently to relieve pain. Fentanyl may also be used for pain control in this setting.
The patient is taken via ambulance to the emergency department where the cath lab has been notified. Depending on the cardiologist’s preference the patient may be loaded with a IIb/IIIa inhibitor such as Integrillin or with Plavix. The patient may receive Heparin while in the emergency department. She is taken to the catheterization laboratory immediately upon arrival of the call team and angiograms are completed. The angiograms are as follows.
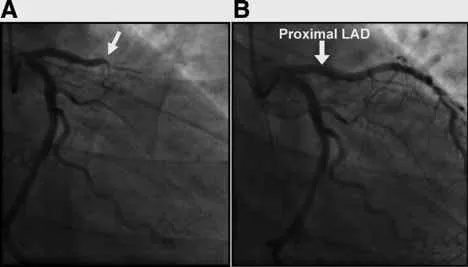
On the left (A), you can see a picture from the patient’s right side that the left anterior descending (LAD) artery is completely occluded. A wire is passed through the blockage and a balloon is inflated restoring flow. (Picture B) You can appreciate the amount of myocardium (heart muscle) that was dying when there was no oxygenated blood reaching it because of the occluded LAD. With flow restored, loss of heart muscle is kept to a minimum.
Test your knowledge
Stay on track!
Would you like a reminder when your ACLS certification expires, plus study tips?
How we reviewed this article
Our experts continually monitor the medical science space, and we update our articles when new information becomes available.
- Current versionMail the author of this pageEmail
- Jan 14, 2023
Copy edited by:
Copy editorsChanges: Fix formatting of the rhythm strip- Nov 13, 2021
Reviewed by:
 Caitlin Goodwin DNP, CNM, RN Caitlin Goodwin, DNP, RN, CNM, is a Board Certified Nurse-Midwife, Registered Nurse, and freelance writer. She has over twelve years of experience in nursing practice.
Caitlin Goodwin DNP, CNM, RN Caitlin Goodwin, DNP, RN, CNM, is a Board Certified Nurse-Midwife, Registered Nurse, and freelance writer. She has over twelve years of experience in nursing practice.- Jun 28, 2017
Written by:
Judy Haluka Judy has helped write or review several medical publications for us. Everything that she works on will clearly include Judy’s name.