Wellens syndrome - ECG case study
 Written by Judy Haluka
Written by Judy Haluka
Changes: Fix formatting of the rhythm strip
This 45-year-old male comes to the emergency department after several days of on again, off again chest pressure. This morning he woke up with 8/10 pain that he describes as “crushing” in nature. It was in the center of his chest but is also causing some discomfort down his arm. It went away after about 30 minutes. It came back just prior to coming to the emergency department. He is currently pain free.
Past eedical history is unremarkable, although he does have a paternal history of coronary disease. His father had his first MI at the age of 48 years. He currently takes no medication except for a multi vitamin.
Exam: The patient is anxious, although pain free. His skin is warm, pale and slightly diaphoretic. His pulses are all strong and regular.
Pulse is 82. Respirations: 22 Pulse Oximetry: 96% on room air. BP: 148/88
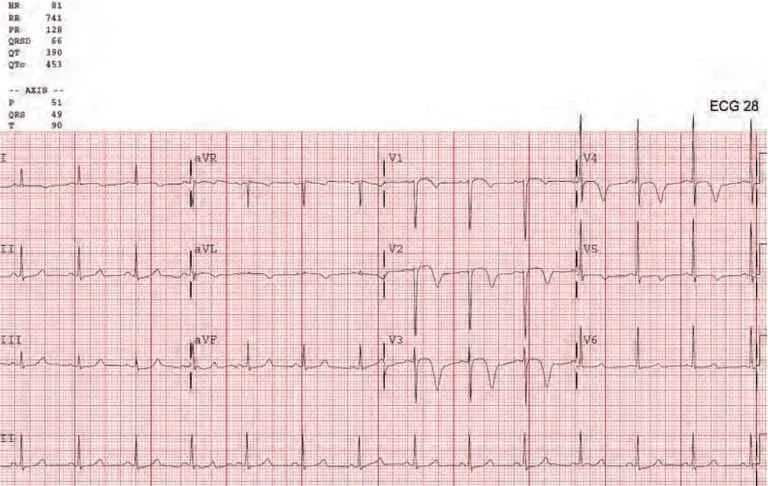
Monitor: Normal sinus rhythm with a rate in the 80’s. His 12-lead ECG is as above.
Are you concerned? What treatment should be started?
This patient’s treatment should include:
- Oxygen therapy, admission to the telemetry unit, and a stress test
- Aspirin, Emergent Cardiac Catheterization
- No immediate treatment is necessary
- Nitroglycerin drip and admission to CCU. Cardiac catheterization electively
You suspect that this patient has
- A significant coronary stenosis
- STEMI
- Stable angina
- Musculoskeletal pain
If this patient is not properly treated he will probably experience
- Inferior wall infarction
- Stroke
- Anterior wall infarction
- There is no way to tell
Discussion: This patient’s immediate treatment should be based on the algorithm for Acute Coronary Syndrome. This should include aspirin (heparin if catheterization is delayed for any reason). He does not require oxygen therapy as he is not short of breath and his oxygen saturation is above 94% on room air.
ECG: This ECG is indicative of Wellen’s Syndrome. The ECG reveals deep T-wave inversion (or biphasic T-waves) in V2 – V4 in a patient who had previous chest pain that has resolved. This is an indication1 of critical proximal LAD disease and requires immediate catheterization and stent placement to avoid infarction. Left untreated, these patients will experience acute anterior wall infarction in the immediate future.
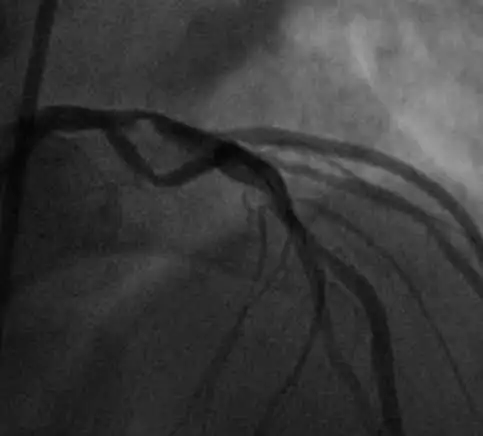
This patient was taken to the catheterization laboratory which revealed the following proximal LAD lesion. A drug-eluting stent was placed resulting in the restoration of normal flow. The patient should do well into the future.
Works Cited
1: Miner B, Grigg WS, Hart EH. Wellens syndrome. StatPearls. StatPearls Publishing; 2021 January. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482490/
Test your knowledge
Stay on track!
Would you like a reminder when your ACLS certification expires, plus study tips?
How we reviewed this article
Our experts continually monitor the medical science space, and we update our articles when new information becomes available.
- Current versionMail the author of this pageEmail
- Jan 14, 2023
Copy edited by:
Copy editorsChanges: Fix formatting of the rhythm strip- Nov 29, 2021
Reviewed by:
 Caitlin Goodwin DNP, CNM, RN Caitlin Goodwin, DNP, RN, CNM, is a Board Certified Nurse-Midwife, Registered Nurse, and freelance writer. She has over twelve years of experience in nursing practice.
Caitlin Goodwin DNP, CNM, RN Caitlin Goodwin, DNP, RN, CNM, is a Board Certified Nurse-Midwife, Registered Nurse, and freelance writer. She has over twelve years of experience in nursing practice.- May 14, 2015
Written by:
Judy Haluka Judy has helped write or review several medical publications for us. Everything that she works on will clearly include Judy’s name.