Posterior wall - ECG case study
 Written by Judy Haluka
Written by Judy Haluka
Changes: Fix formatting of the rhythm strip
This 78-year-old woman is wheeled into the emergency department by her son because she is too weak to walk. She is normally ambulatory and energetic. Over the past hour or so she has felt “extremely weak and tired.” She states, “my whole body hurts and I just want to go to sleep.”
Past Medical History: Severe arthritis, CVA 10+ years ago, and insulin dependent diabetes.
Medications: “a couple of heart pills” and insulin. She is supposed to take aspirin daily but hasn’t for some time as it bothers her stomach.
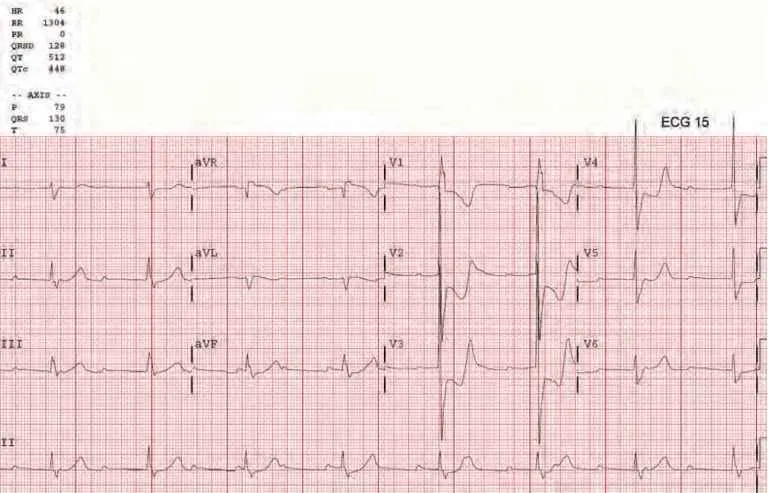
Exam reveals an “ill looking” woman who is slow to respond. She is appropriate with her answers but very sluggish. She is pale and slightly diaphoretic. Her radial pulses are absent, carotids are palpable at a rate of approximately 40 bpm. Her blood pressure is difficult to hear, but registers 68/40 on the automated cuff. The pulse oximetry will not pick up on her finger. Her ECG is above.
- This patient’s cardiac rhythm is:
- Sinus rhythm
- Third-degree heart block with a junctional escape response
- Third-degree heart block with a ventricular escape response
- Sinus rhythm with first-degree block
- This ECG Reveals:
- No STEMI or ischemia present
- Acute inferior wall infarction
- Acute anterior wall infarction
- Acute posterior lateral wall infarction
- Immediate treatment should include:
- Oxygen, transcutaneous pacing (while obtaining IV Access), aspirin (ASA ),and activation of the cardiac cath lab
- There is no immediate treatment necessary, continue diagnostic testing.
- Oxygen, Lopressor, and activation of the cardiac catheterization lab
- Oxygen, Amiodarone and activation of the cardiac catheterization lab
- The correct answer is third-degree heart block with a junctional escape response. This woman’s rhythm is complete heart block. The heart rate is maintained in the 40’s and the QRS complex is narrow because the underlying rhythm originates in the AV Node (Junctional Escape Rhythm) rather than the ventricle which would result in a much slower and wider rhythm.
Anytime a patient presents with extreme bradycardia, DIES should come to mind to assist with diagnosis. Drugs Ischemia/Infarction, Electrolytes, Sick Sinus Syndrome.
- In our patient’s case, we are dealing with an acute infarction. This ECG reveals a posterior wall infarction. Note the ST depression in V1-V3.
The following changes in V1-3 suggest posterior MI:
- Horizontal ST depression
- Tall, broad R waves (>30ms)
- Upright T waves
- Dominant R wave (R/S ratio > 1) in V2
- This patient’s symptoms are most likely caused by her bradycardia. Treatment of this patient should include.
- Administration of oxygen. The pulse oximeter is not reading (probably because of her hypotension) therefore you must assume that oxygen is needed and administer it.
- Aspirin (ASA) administration
- Transcutaneous pacing can be used to increase the patient’s heart rate and blood pressure. This is especially true because there is no IV access yet in this patient.
- The Cardiac Catheterization Laboratory should be notified as soon as possible as this is a STEMI and the goal must be to open the vessel.
Test your knowledge
Stay on track!
Would you like a reminder when your ACLS certification expires, plus study tips?
How we reviewed this article
Our experts continually monitor the medical science space, and we update our articles when new information becomes available.
- Current versionMail the author of this pageEmail
- Jan 14, 2023
Copy edited by:
Copy editorsChanges: Fix formatting of the rhythm strip- Dec 5, 2021
Reviewed by:
 Caitlin Goodwin DNP, CNM, RN Caitlin Goodwin, DNP, RN, CNM, is a Board Certified Nurse-Midwife, Registered Nurse, and freelance writer. She has over twelve years of experience in nursing practice.
Caitlin Goodwin DNP, CNM, RN Caitlin Goodwin, DNP, RN, CNM, is a Board Certified Nurse-Midwife, Registered Nurse, and freelance writer. She has over twelve years of experience in nursing practice.- May 11, 2015
Written by:
Judy Haluka Judy has helped write or review several medical publications for us. Everything that she works on will clearly include Judy’s name.